

Non venereal syphilis also called endemic trepanomatoses are chronic infectious conditions related to some treponemas which are very similar to the one of venereal syphilis. Humans are their only natural hosts. These diseases are distributed across rural Asia, Africa and Central America and it is in general accepted that tens of million people were at risk around the world at the turn of the twentieth century.
In all territories where it was in charge, the Colonial Medical Corps laid out plans for the diagnosis and the treatment of the people afflicted in order to achieve the control of these endemic conditions.
In 1955 The Major Endemic Diseases Service started to be involved in this scheme and led a decisive fight against these conditions with mass campaigns just after it had been found that penicillin therapy was an extraordinary efficacious treatment of such conditions.
The outcome is an impressive one with a declining number of patients across the world.
ENDEMIC TREPANOMATOSES OR NON VENEREAL SYPHILIS
Physicians failed at first to identify that all syphilis cases in tropical countries were not sexually transmitted. Venereal lesions of syphilis were well known in Europe. In continuation of Bordet’s previous scientific works, Wasserman developed a serological test in 1906 for the diagnosis of trepanomatosis infection. In many tropical countries many native adults tested positive but they denied any past history of syphilis, despite of the fact that it is always difficult to ascertain that it was true, and they did not display any well acknowledged symptom of syphilis. On the other hand many prepubescent children tested positive also. At first this could not be understood and the possibility of hereditary or congenital transmitted syphilis was considered and consequently individuals who had tested positive had to undergo a course of treatment. Later on the idea of non sexually transmitted syphilis started to be progressively accepted.
Three different conditions are acknowledged as non venereal trepanomatoses : yaws, endemic syphilis also named bejel and pinta :
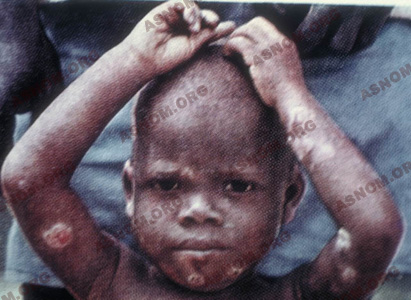
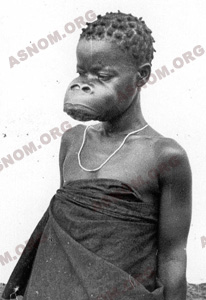
– Yaws is the one with the most remarkable cutaneous and mucosal features. The first lesion goes most of the time unnoticed and the typical cutaneous finding is a sore also called frambesia which is an itching, granulating and oozing ulcer with a thin scab at the top. This lesion is found in variable numbers all over the skin but mostly in moist areas. On palms and soles the hard skin is penetrated and this results in ulcerated and very painful sores known as crab yaws. Bone lesions show up later, most of the time they are located on long bones and especially on shinbones and they result in crippling deformities and in the late stages, in mutilations.
– Bejel : Clinical features of Bejel are not conspicuous as lesions are located on mucosas of the mouth and sometimes also of the genitals. They consist in small ulcers, called mucosal patches, which are found in the mouth on the back of the lips and on the cheeks. Cutaneous lesions in the shape of nodules or gummas are rare and there is no associated deterioration of the patient’s general condition. During the late stages of the disease there is also a rather mild bone involvement.


– Pinta or carate features lesions of the skin which can be either bluish, erythemetous or discolored mimicking a painting hence the name of this disease. These lesions are distributed all across the skin in different places and there is no noticeable late clinical involvement of any other organ.
Distribution of these diseases across the world is a remarkable one and is different according to the disease which is considered :
Yaws is a disease which is found in hot and humid regions such as forests and coastal plains and as the saying goes "Yaws starts where the road comes to an end". Bejel is found in dry and arid areas of the Middle East and Africa. Pinta is found only in Central and South America.
Contagion depends on climates : on the one hand with a humid climate exuding yaws lesions contribute the transmission of pathogens and on the other hand in drier savannah regions, lesions which are less prone to oozing, are less contagious, except for those which are located on mucosae or in moist areas such as lips or armpits. But in many instances patients with these diseases remain symptom free and can only be diagnosed through serological testing.
ANOTHER TREPONEMATOSIS : VENERIAN SYPHILIS
A sexually transmitted disease, venerian syphilis is the most notorious and the only one found the world over. If not attended to, it triggers severe conditions (which can be lethal), most particularly of the aorta and the nervous system. And it can be transmitted to the foetus which will be affected by a congenital syphilis.
This universal type is also found in the tropics, mostly in cities and ports.
COMMON AND DISTINCTIVE CHARACTERISTICS OF THESE ENDEMIC TREPONEMATOSIS
All treponemasosis have in common :
– They are all triggered by a similar germ, the treponema, identical to that of syphilis,
– the same antibodies are found in the blood, therefore an identical serology is applied for these affections and syphilis,
– they respond to penicillin as well as to other antibiotics.
On the other hand, these treponematosis are different from syphilis because :
– They are not sexually transmitted, and occur very early, between 2 and 10, generally by direct contact with wounds, or superficial oozing scratches of another child. Poor hygiene (shortage of water, lack of soap), promiscuity, and distance from a health clinic favour the spreading of this contagion.
– These diseases are mostly found in rural areas and affect a very large percentage of individuals. We can talk of a "major endemic".
– They haven’t been observed in temperate climates, solely in tropical or sub-tropical countries,
– they are not transmitted from the mother to the foetus. As opposed to syphilis which is transmissible trom the mother to the foetus. The child is then affected with a congenital syphilis.
– They do not result in visceral or nervous complications but sometimes affect the bone structure. They are not an obvious cause for a spontaneous miscarriage.
For a patient who has a positive serology which is identical to that of the classic venerian syphilis, the problem is not to mistake these affections with those of the latter the evolution of which is more serious. Syphilis is without any doubt the most notorious treponematosis and the most universally spread. In the tropics, it is mostly observed in urban areas and in ports. It is transmissible through sexual intercourse. If not treated, it is responsible for very severe symptoms that appear later, which are often lethal, specially when affecting the cardio-vascular and neuro-psychiatric systems. None of these late symptoms are observed in the course of the evolution of endemic treponematosis.
SCREENING AND THERAPY
At first, colonial physicians who came across lesions due to treponemas used the medications which were then available. During the nineteenth century, sodium iodide was the core medication and it should be acknowledged that it was kind of therapeutic for old gummas and nodules related to treponematoses. In the nineteen fifties old Toucouleur people along the Senegal River used to report to nurses and to make requests, for potassium iodide, which they named "ripotassion" in order to alleviate pains which they had at night.
As of 1910 arsenical compounds such as novarsenobenzol, arsenones and sulfarsol started to be used successfully but they had deleterious side effects such as neuritis and jaundice. Bismuth became available after 1920 : efficient and better tolerated than arsenical compounds but still it displayed toxicities for kidneys and mouth mucosal membranes.
Meanwhile Botreau-Roussel* who had an especially comprehensive knowledge of yaws lesions and of its possible maiming complications devised appropriate corrective surgical procedures.
Notwithstanding these efforts this endemic disease was not contained as the only patients who could be treated were the ones living close to a medical facility where most of the time they reported with maiming lesions occurring during the late stage of the disease when there is only a very small risk of contagion left. Most of the really infectious patients could not take advantage of any therapy. Moreover no one was then aware that asymptomatic contacts had also to be treated as they were at risk of having a latent or incubating infection and as they constituted the main reservoir of infection.
The use of Penicillin which was started in 1941 was real a breakthrough when it was found that its efficacy against treponematoses was together an outstanding and extremely well tolerated one. But it is only much later that mass campaigns could be contemplated and then undertaken.
THE DECISIVE BATTLE
When he was at the head of the biology department of the Muraz Centre in Bobo Dioulasso, Upper Volta, which was the Headquarters of the SGHMP, J. Ridoux* had the opportunity to attend the second international conference in Nigeria (1955) during which the severity of this social and economical issue was correctly assessed. A codification of the methods which had to be implemented for screening, treating and monitoring was also made. Mobile clinical and serological screening teams were set up according to Jamot’s doctrine.
At the head of the SGHMP, Masseguin* and then Richet* put in place the logistics while those who had been assigned to the head of this scheme such as Ridet* and Causse* had to devise the strategy for the fight and also had to provide medical teams with the equipment and technical help which they needed on the field of action.
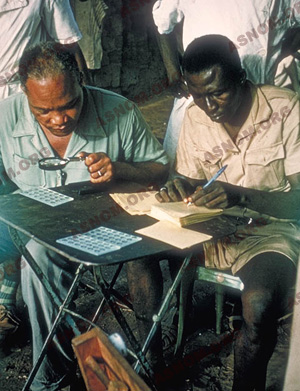
A team included a physician, African nurses and laboratory technicians who all over their designated territory surveyed with a serological test all age groups, in every village and in every section of large cities. On the same day blood samples were taken and serological tests subsequently carried out.
Populations who had been given prior notice and relevant information had to gather on the appointed day and the team screened and treated between one hundred and one hundred and fifty people every day, one family at a time. They used to work without making any break to make sure that physical screening, blood sample collection and subsequent treatment of patients could all take place within the same day.
Preliminary results of these surveys confirmed the importance of this issue as in Sub Saharan Africa, very often over 20 % of the patients with yaws happened to have infectious lesions, 10 % were disabled with mutilating lesions and 70 % to 80 % were asymptomatic carriers (positive serological test but no symptoms).
These surveys were conducted in geographic areas with a high level of endemicity before undertaking any campaign of treatment for masses.
Hence the organization of mobile teams equipped with 2 or 3 four-wheel drive vehicles, with fuel, food, water, sleeping gear, etc…
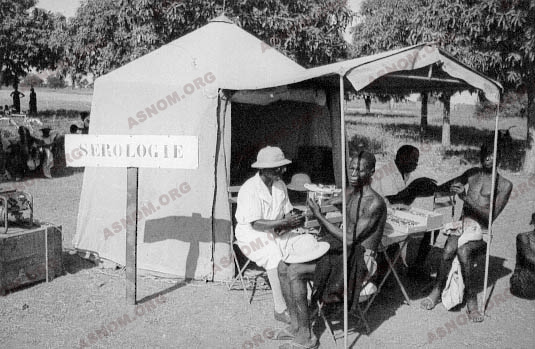
These mobile teams work under tents which are equipped with the essential machines (extractors, double-boiler, agitator, and of course a power generator running on petrol). All these equipments as well as those necessary for the personnel’s daily needs : beds, kitchen, water purifying unit, must be installed, and taken down every day to go to the next gathering place which often is quite a few hours away.

The names of around one hundred Colonial Army young medical officers and also those of several hundred African nurses are connected with this undertaking. Nomadic medical teams deserve special merit as they used to keep track of tribes of herdsmen in the Sahel or the desert who drifted with rainfalls and their short-lived subsequent grazing grounds.
WHO’s Treponematoses Division was headed from 1972 to 1985 by Causse* who made a supervision of this mass campaign of treatment.
The efficacy of the initial treatment was assessed through follow up surveys which gave individuals who had missed the previous checks the opportunity of being screened and treated. But above all, this was an excellent opportunity to promote protocols securing the stabilization of the results which had been achieved. Part of this work of stabilization was done together with local health facilities (AMI) which were mostly in charge of providing primary health care and this cooperation provided that any local epidemic outbreak could be diagnosed and swiftly eradicated. Moreover health information messages could be passed to populations with incitements to be treated and to improve their corporeal standards of hygiene.
CAMPAIGN OF TREATMENT FOR MASSES
Therapy came together with advices regarding corporeal hygiene of individuals but also general hygiene of communities.
Before the availability of penicillin there were several therapeutic protocols with the use of arsenical medications but all of them provided varied and unconvincing results.
In 1943 the first patients with yaws who could be treated with penicillin were prescribed a one to four day long treatment with a dose ranging from 250 000 to 600 000 units. Results were quite spectacular and lesions subsided all the better since they were recent ones. Later slow release varieties of penicillin became available which secured sufficient antibiotic seric levels over a 10 to 15 day long period of time such as :
– Procaine-Penicillin in an oily solution added with alumine monosterate known as PAM penicillin, which provided inconstant results according to the batches.
– Dybenzyethylene-diamino-dipenicillin G known as Benzathin-Penicillin was developed in 1951. It is active over a period of time which is twice as long as for PAM. So that a single intramuscular injection of 2 400 000 units secures the killing of treponemas over the next 22 days.
Those who had to be treated, were of course the patients and also other individuals who had been in contact with them so that in some instances it had to be decided to implement the treatment for the whole population.
Just a few hours after treatment has been started the most recent lesions are no more infectious and are completely healed after eight to ten days but the healing of older lesions or of "crab yaws" lesions takes usually longer. Depending on the time which had elapsed between the onset of the disease and the treatment, serologic tests will not perform identically.
According to the recommendations of the mobile team and moreover with the UNICEF technical and material support it was decided to implement an efficacious treatment for entire populations and treatment protocols were set up according to levels of endemicity :
– Hyper-endemic areas : Over 10% of clinical cases in a population with a positive serological test for nearly 100% of the people. The whole population had to be treated with the use of a slow release penicillin as those asymptomatic individuals with a positive test were considered as experiencing either a latent phase or the incubation period of the disease. A single injection of 2.4 M. i.u. was administered to adults and 1.2M.i.u. to children.
– Meso-endemic areas : 5-10% of clinical cases : all of them were treated according to the same protocol, all children under 15 years of age were also treated as they were considered as the primary infection reservoir with all obvious contacts of patients.
– Hypo-endemic areas : Less than 5% of clinical cases, treatment of clinical cases and of contacts.
STOCK OF THE ACHIEVEMENTS
Several million people were screened and treated during the early years of this mobile campaign. The results are quite spectacular as recent contagious cases have nearly totally disappeared now in populations which have been screened while their serological tests are still positive but this sero-conversion remains beyond any therapeutic possibility.
These diseases are receding around the world but there is stil a need for watching out to prevent or eradicate any sudden outbreak which can occur unexpectedly. Nevertheless penicillin therapy is still in use as this medication which has remained fully active over the years is inexpensive and its administration protocol is easy to implement. The only remaining issues are on the one hand the accurate recognition of these diseases and on the other one the intention of reaching out for patients so that they can be cared for and subsequently cured.

For further information :
– Hackett J.C. : Nomenclature internationale des lésions pianiques O.M.S., série monographies n° 36.
– G. Causse, G.M. Antal : Manuel des tréponématoses endémiques . O.M.S. 1985.
– Diop Mar I. Marchand J.P. : Diagnostic des tréponématoses chez des africains. Conc. Méd. 1976,98,17,2569-2586.